The key-question for Elderly people: not do you live alone but: do you feel alone? Final Q&A
Some speeches:
Mental Health and the Wellbeing of Older People (Most Reverend Noel Simard, Bishop of Valleyfield, Québec, Canada)
I- FUNDAMENTAL ETHICAL VALUES AND PRINCIPLES
- The Inherent Dignity of the Elderly Person
- i) The elderly person remains a person
ii) Must continue to becoming a person
iii) As social being, needs the community
• It is essential to include spirituality and religion in the healing process in order to improve the well-being and the quality of life of the elderly with a mental problem or disorder,
• « What is good for the soul may also be good for the body,
• A holistic approach for health presupposes a holistic concept of the person, an integration of care, a Covenant of care, compassion and love,
• An ethics of frailty is necessary to learn about the meaning of dependency and vulnerability, and to develop human relationship based on solidarity, reciprocity and compassion.
Mental Health of the Elderly from an Islamic Perspective (Professor Mohammed Ghali)
•Cannot be separated from the larger Islamic moral framework; •Individual dimension (in case of competence); •Theological; •Juristic; •Moral/spiritual; •Actualization of beautiful names and attributes of God; •Role models and examples in the scriptural sources; •Continuous moral/spiritual development/cultivation; •Social dimension (particularly with lack of competence); •Collective and participatory framework; •Family relationships; •Medical team; •Broader social connections/implications/stakeholders.
•Importance of underlying conceptualization of oneself and one’s place in the universe; •Role of religion and culture; •Paying special attention to the role of mental health in elderly care; •Individual and collective responsibilities; •Incorporation of the elderly perspective; •Role of family members; •Role of specialized medical staff; •Involvement of various stakeholders; •Development of and continuous revision of special/specific protocols; •Should be based on collective reflections and deliberations; •Should cover various physical, social, religious, and financial needs; •The sick; •The elderly; •The dying.
Christians and Muslims agree about the social importance of Elderly people. They are a living memory. Take care of their economic, social, spiritual, health situations.
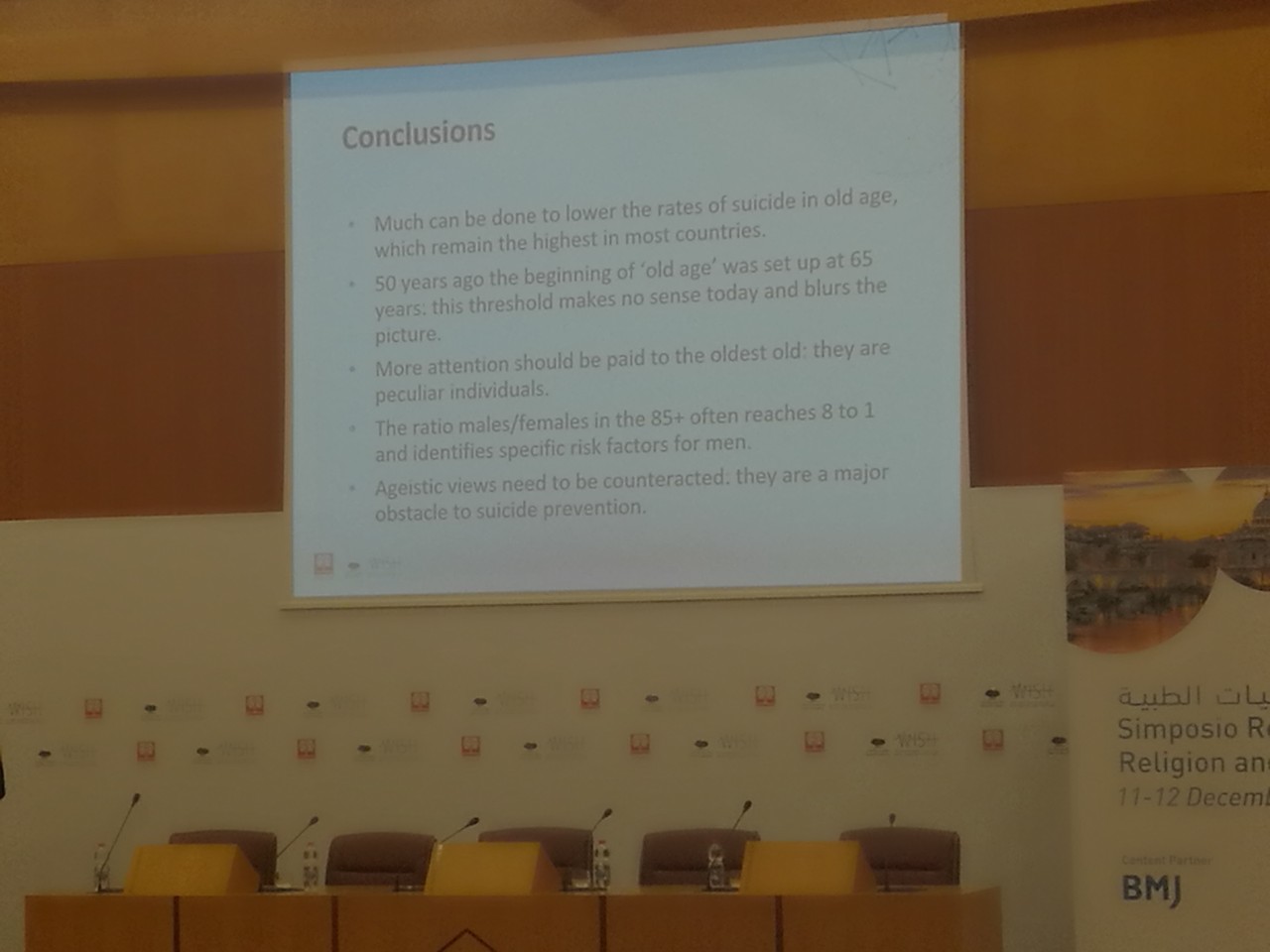
Safeguarding the Mental Health of Elderly patients receiving Palliative Care (dr. Ferdinando Cancelli)
•Ensure that patients and their families are offered regular opportunities to talk to staff about their changing situation and concerns. •Use the patient’s name as they like to be addressed; •Make time for the patient; •Create the opportunity to talk about spirituality; •Always seek to enable a patient to express their preferences; •Offer a private room for the patient; •Be clear about the relative benefit and need for sedative medication; •Ask the patients/family if they have any particular religious beliefs; • Consider offering the sacrament of communion and involve the chaplaincy team as soon as possible.
•Depression remains underdiagnosed even in institution: too often we forget that depression is in no way a consequence of normal aging; •Suicide remains an important cause of death for the elderly person (2010: 2873 people older than 65 yrs, 30% of total suicide); •In the older than 85 years group, the prevalence of suicide is twice as high as that of the 25-44 age group; •Men older than 95 yrs of age kill themselves on average 10 times more than the general population; •Safeguarding the mental health of elderly patients receiving palliative care is the better way to avoid euthanasia and assisted suicide.
•«I like this place because death, when it comes, still finds us alive!»
The bridge of Love: dementia (Prof. Marco Trabucchi)
We must improve our ability to care both at the personal and social levels, considering that a dementia cure is far away.
In the world there are 4 kinds of persons: Those who cared 4 someone Those who are caring 4 someone Those who will care 4 someone Those who needed care or will need it.
Other subjects: "I think we need to talk WITH elderly people not just ABOUT them". Dr. Mohammed Ghaly from @HBK
Prof. Paulina Taboada: "Treating spiritual issues as part of a checklist in the same way as physical symptoms does not allow one to adequately tackle them, as they are more encompassing. Spirituality can contribute in it's own right to healthcare".
Abp. Paglia closing remarks: "We are speaking about all believers on all religions, not just leaders. Otherwise we would take away from the people most in need in love and place everything in the hand of experts". Make palliative care a required part of all medical training, and 4. prioritize the development of pediatric palliative care. We have a long way to go and we are just at the beginning. "We are speaking about all believers on all religions, not just leaders. Otherwise we would take away from the people most in need in love and place everything in the hand of experts".
“Suicide is a request for love that hasn’t been answered”. What a powerful closing statement
"Faith needs to be integral to holistic care" - Final remarks from Archbishop Vincenzo Paglia and Sultana Afdhal at the conclusion of the meeting.